Pain Gating
To understand pain gating, we must first understand how pain works. Pain is essentially a warning system in the body that lets your brain know something is wrong. Think of it as the body's car alarm when something's not right. When experiencing pain from an injury, pain signals are sent to the spine, which is sent to the brain. The brain then decodes them into the feeling of pain.
Pain gating is a theory created by Ronald Melzack and Patrick Wall in the early 1960s. Pain gate theory explains how nerves perceive pain, and touch impedes that perception. Essentially, the theory states that there are "nerve gates" at the end of your spine that control if pain signals are allowed to pass to the brain to be decoded. There are two types of nerve fibers, small (pain fibers) and large (fibers for skin senses such as touch and pressure). These fibers carry information from the area of pain to the spine.
When small fiber activity is more abundant than large fiber activity, the pain gate is open, allowing pain to be transferred to and decoded by the brain. However, the pain gate is closed when large fiber activity is more robust than small fibers. This does not allow pain nerves to be sent to the brain (i.e., no pain!).
Pain gate theory explains why we rub or shake injuries after they occur. By rubbing or shaking the injured area, we're creating more large fiber activity, which diminishes small (pain) fiber activity, thus reducing the sensation of pain.
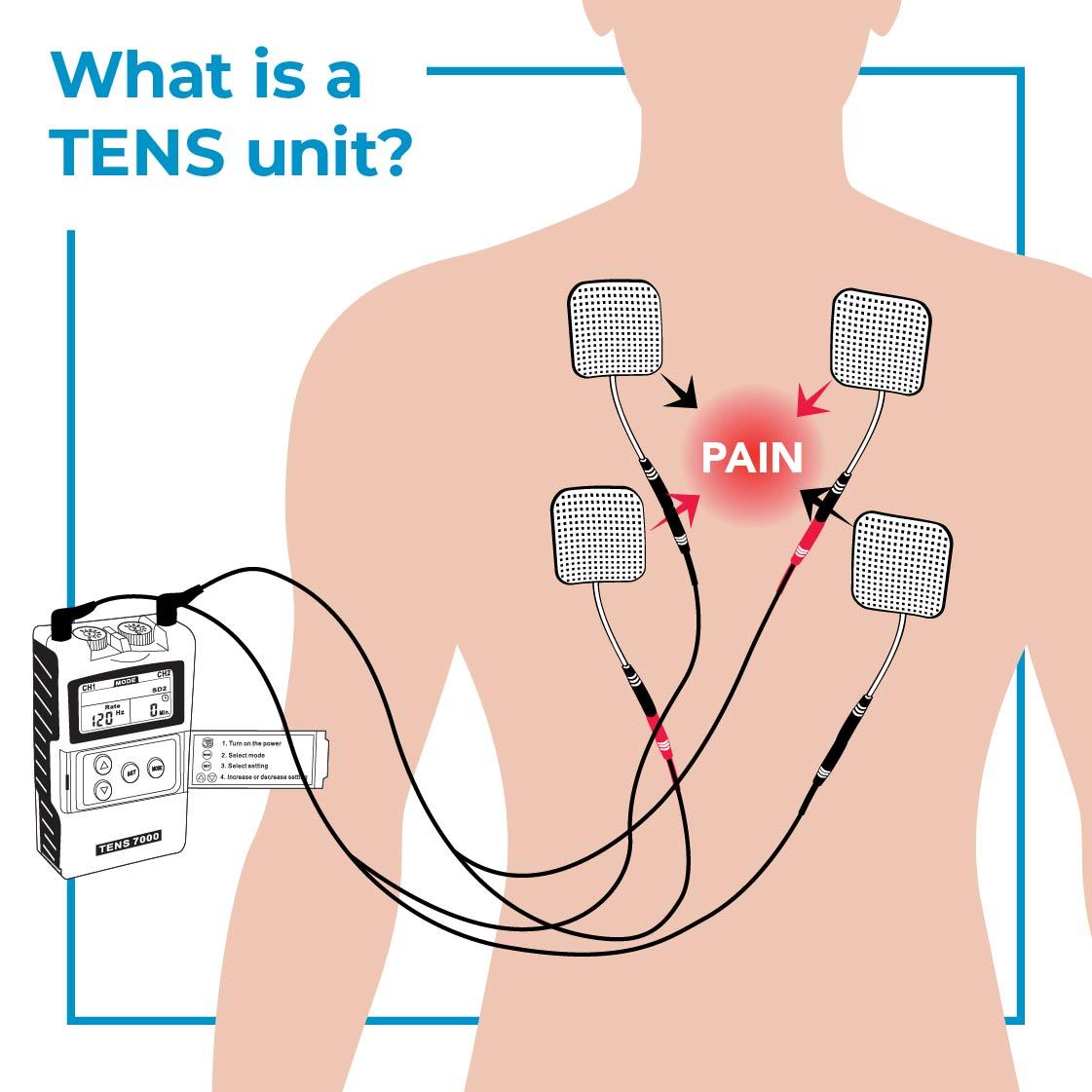
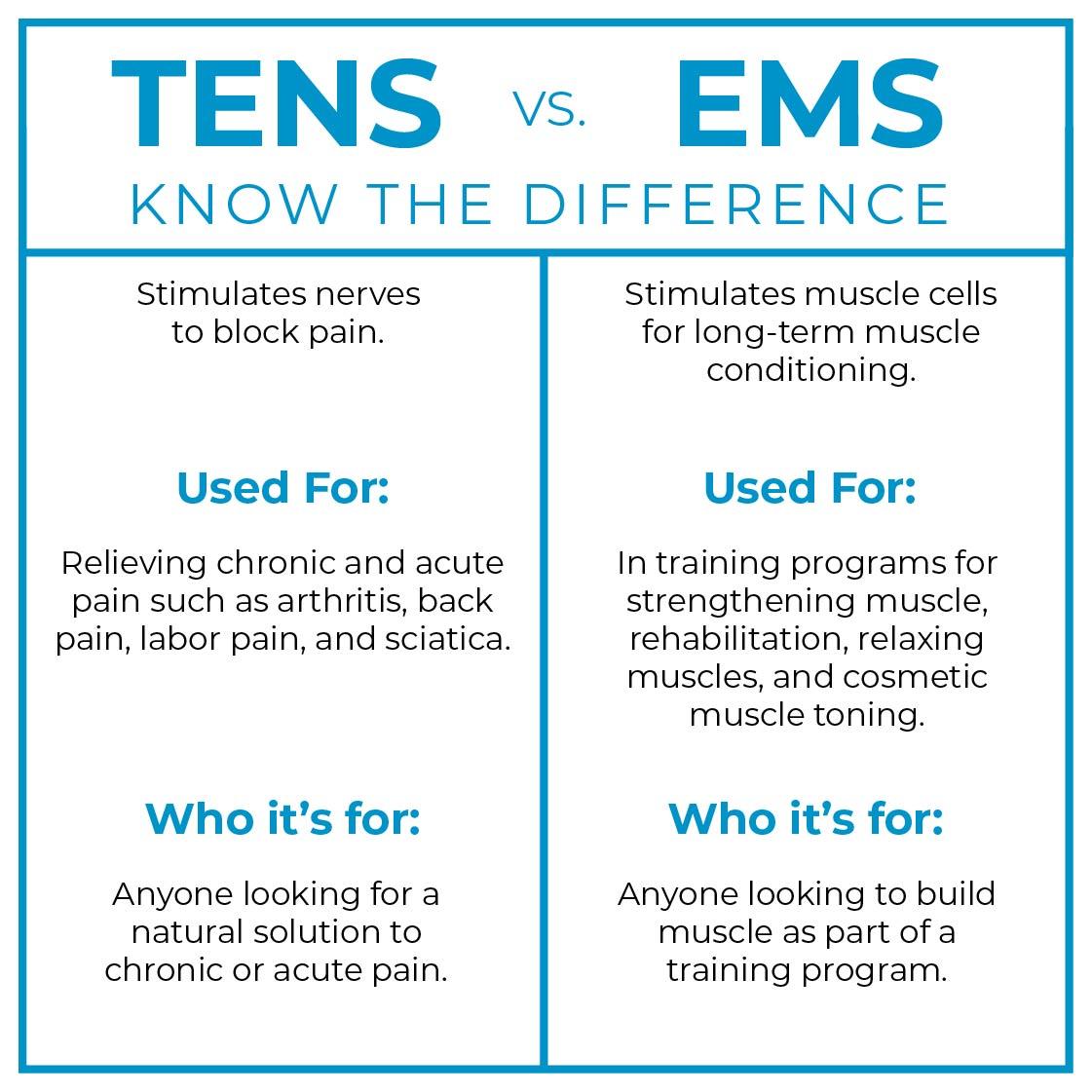
A TENS unit activates large fibers to overpower small fibers by creating a tingling or massaging sensation to close pain gates. The tingling/massaging sensation doesn't allow pain fibers to transmit painful feelings to the brain. In short, the pain gets temporarily blocked.